GentleMax Pro Plus®
755 nm Alexandrite Laser Hair Removal in a Patient with Recurrent Boils
Ponyai Katinka, MD, PhD; Fanni Baranyai, MD; Kinga Raduly, Medical Assistant Dermart Buda Clinic, Budapest, Hungary
Introduction
A boil (furuncle) is a necrotizing form of folliculitis (inflamed/ infected hair follicle that forms a pustule or erythematous papule) with involvement of the subcutaneous tissue. It is mostly caused by the bacterium Staphylococcus aureus, resulting in a painful bump that forms under the skin.1 These bumps usually start as reddish or purplish, tender bumps which quickly fill with pus, growing larger and more painful until they rupture and drain. They often occur in areas of dense hair that experience friction and sweat, such as the back of the neck, face, armpits, waist, groin, thighs, or buttocks. Predisposing factors include obesity, diabetes, prolonged sitting, wearing tight or irritating pants, and immunodeficiencies.1 The GentleTM 755 Alexandrite laser has been shown to resolve preexisting hidradenitis suppurativa (HS) lesions and prevent new eruptions in various anatomic areas.2 The laser has also been reported to improve follicular plugs, perifollicular erythema, and perifollicular hyperpigmentation in keratosis pilaris3 and result in long-term hair removal.4 In addition, laser treatment has been shown to reduce the skin’s bacterial count of Staphylococcus aureus.5 In this case spotlight we present a patient with recurrent boils treated with the Gentle 755 nm Alexandrite hair removal laser.
Case study
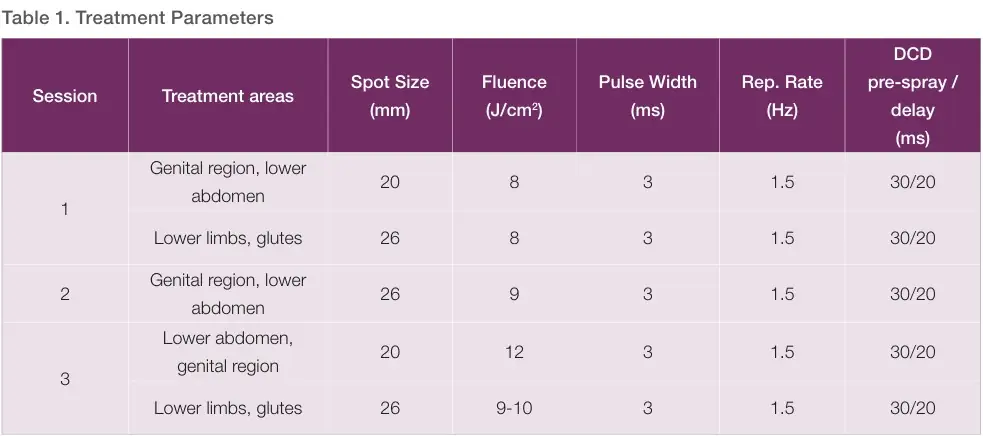
A 36-year-old female patient, with Fitzpatrick Skin Type (FST) III, who is a smoker but with no serious illnesses in her medical history, presented with boils. The patient suffered from inflamed, slow-healing furuncles in the genital region, gluteal region, and lower extremities since the age of 16 years, which healed with residual scarring. Prior to the development of furuncles, the subject experienced fever, chills, and malaise as prodromal symptoms. She had seen several dermatologists and undergone multiple 2‑to 3‑month cycles of systemic therapy of tetracycline, clindamycin, and isotretinoin therapy. She experienced temporary improvement, but her symptoms returned, even while taking the medications. The patient also tried Octenisept® antiseptic solution (oktenidin-dihidroklorid/fenoxietanol) for local external disinfection. Diagnoses and clinical examinations yielded negative ANA (antinuclear antibody) panel results, and routine laboratory f indings showed no significant abnormalities. HIV, hepatitis, and syphilis serology revealed no notable findings. Chest X‑ray, abdominal ultrasound, gynecology, laryngology, and dentistry were all negative. General bacteriological and fungal cultures taken from the furuncle showed no pathogenic growth. Punch biopsy histology indicated acute neutrophilic inflammation. The patient was prescribed doxycycline antibiotic, vitamin D, and clindamycin gel topically. Despite temporary improvement, her symptoms recurred. Biological therapy was considered within the framework of clinical examination with a provisional diagnosis of HS, but due to atypical symptoms present on the legs, the patient could not be included in the trial. The subject received a series of 3 GentleMax Pro Plus® 755 nm laser treatments* (with 6‑week intervals between sessions) to the lower limbs, abdomen, genital area and buttock (Table 1). Before the procedure, the areas were evaluated and disinfected with Octenisept®. Treatment was performed using a single pass except in areas of inflammation or open lesions, where a single pulse was applied in the center followed by 4 – 5 pulses surrounding the lesion with 30 – 40% overlap. Epidermal cooling was applied using the Dynamic Cooling Device (DCD®) to protect the skin and enhance comfort with 30 ms duration and 20 ms delay (30÷20 ms). The clinical endpoint was perifollicular edema and mild erythema around the hair follicles.

Cool compresses were applied immediately after each treatment, followed by panthenol foam. Panthenol was also used locally twice daily for an additional five days. Patient was advised to keep the area cool post-treatment and to avoid strenuous exercise, saunas and similar activities for at least five days. Additional guidance included to avoid sun exposure 4 – 6 weeks before and after treatment and to use SPF 50 sunscreen between sessions. Use of clindamycin gel was permitted as needed. It was also advised to avoid bleaching and waxing hair for 6 weeks prior to and throughout treatments.
Results
Subject improvement was evident even after the first treatment, with a reduction in inflamed nodules. The subject did not feel any pain during treatment and the downtime was only one day, until the perifollicular edema resolved. The patient’s general mood improved. After the third treatment, the inflamed furuncles in the lower extremities had resolved remarkably (Figure 1). The patient proceeded with two additional treatment sessions and expressed high satisfaction with the treatment outcomes.
Summary
The 755 nm alexandrite laser primarily targets melanin (absorbing chromophore) in hair follicles, making it an effective tool for long-term hair reduction. Similar to previous applications in chronic inflammatory skin conditions such as HS2, the GentleMax Pro Plus 755 nm laser hair removal treatment appeared to support improvement in the subject’s furuncle-related lesions and overall skin condition. Targeting the hair follicle may help reduce the factors that contribute to recurrent furuncles or folliculitis, as these conditions often begin with inflammation in the follicle. Further studies may be needed to substantiate these results.
References
2. 3. 4. 5. Ioannides D, Lazaridou E. (2023). Furuncles and Carbuncles. In: Katsambas AD, Lotti TM, Dessinioti C, D’Erme AM. (eds) European Handbook of Dermatological Treatments. Springer, Cham. Sidhom S, Petry SU, Ward R, Daveluy S. Treatment of hidradenitis suppurativa with 755-nm alexandrite laser hair removal: A randomized controlled trial. JAAD Int. 2024 Apr 24;16:239 – 243. Li M, Bai Y, Duan Z, Yuan R, Liu X, Liu Y, Liang X, Wu H, Zhuo F. Efficacy and Safety of Long-Pulsed 755-nm Alexandrite Laser for Keratosis Pilaris: A Split-Body Randomized Clinical Trial. Dermatol Ther (Heidelb). 2022 Aug;12(8):1897 – 1906. Tugba Altunel C, Pelin Kartal S. Reconceptualizing the permanence of alexandrite laser hair removal results: a long-term follow-up study. J Cosmet Laser Ther. 2020 Nov 16;22(6 – 8):271 – 274. Fazel Z, Majidpour A, Behrangi E, Fathizadeh S, Nokandeh M, Atefi N, Ghassemi MR. Using the Hair Removal Laser in the Axillary Region and its Effect on Normal Microbial Flora. J Lasers Med Sci. 2020 Summer;11(3):255 – 261.